Download The Dundee coronary risk-disk for management of change in ... and more Study notes Cardiology in PDF only on Docsity!
The Dundee coronary risk-disk for management of change in
risk factors
Hugh Tunstall-Pedoe
Abstract Objective-To devise a simplified system for grading and monitoring modifiable coronary risk in primary care, to be used with an action plan. Methods-The risk equation came from 5203 men aged 40-59 in the United Kingdom heart disease prevention project, wyho had 331 coronary events over five years; the p6pulation rank (reading 1-100) was obtained by scoring 10359 participants in the Scottish heart health study. Calculation of rank was embodied in the Dundee coronary risk-disk; the formula was tested against the Whitehall study; disk and action plan were evaluated in primary care. Results-The system measures modifiable coronary risk from smoking, blood pressure, and blood cholesterol concentration (^) by a (^) sex and age related rank running from (^1) (high risk, priority action) to 100 (low risk, general advice). The formula predicted outcome acceptably in the Whitehall study and is built into a circular slide rule. Only eight (11%) of 76 general practitioners and practice nurses surveyed already used risk factor scores. After evaluation most thought they should use one and proposed to incorporate the Dundee coronary risk-disk and the associated action plan into their routines. Conclusion-The Dundee coronary risk-disk readout of Dundee rank, standardised on a scale of 1 to 100 by age and sex, is a simple, valid means of assessing and monitoring modifiable coronary risk. It puts single risk factors (such as cholesterol concentration) in perspective and can aid selective testing. Understood by medical staff and patients, it should improve the efficiency and effectiveness of the high risk approach to coronary prevention.
Cardiovascular Epidemiology Unit,
Ninewelis Hospital and
Medical School, Dundee DD1 9SY Hugh Tunstall-Pedoe, MD, director
BM 1991;303:744-
Introduction
In 1989 the Coronary Prevention Group and the
British Heart Foundation convened a (^) working group
(chaired by Professor Geoffrey Rose) to draft an action
plan for preventing (^) coronary heart disease in (^) primary care. They asked me to devise a new system for scoring
risk factors to be used with it, a system that could be
generally adopted as those currently available are not
widely used.
The new system should apply to men and women
aged 35 to 64; emphasise major modifiable risk factors;
enter risk factor values directly; be compatible with
selective cholesterol testing; relate to population
distributions; and be based on published British data.
This paper describes the Dundee score; its simplified
derivative, the Dundee rank; the incorporation of
score and rank into the Dundee coronary risk-disk;
and the results of validation and evaluation in primary
care.
Methods The Dundee score (^) was based on the five year follow
up for^ coronary mortality and^ non-fatal^ myocardial
infarction (^) (331 events) in 5203 men (^) aged 40-59 in the
United Kingdom heart disease prevention project.'
Smoking habit, blood pressure, blood cholesterol concentration, and age were entered into the multiple logistic function,2 but subsequently age was set to 50 to generate a relative risk score confined to modifiable factors. The Dundee rank was derived by calculating the Dundee score for each of the 10 359 men and women aged 40-59 in the Scottish heart health study.3 The distribution by sex was defined in centiles and (^) renamed Dundee rank, running from 1 (highest modifiable risk)
to 100 (least modifiable risk). Dundee score and rank
were re-examined in the Scottish MONICA population
(aged 35-64),4 making adjustments for women. The Dundee (^) coronary risk-disk, a circular slide rule analogue of the^ multiple logistic function calculation for risk and rank was made; it consists of two disks and a pointer. Risk factors are entered from one disk and the resultant Dundee score and rank are read off the second.
Validation-The formula was used to predict deaths
after five and 10 years in 15 395 male civil servants aged
40-59 in the Whitehall study.
Testing in pnimary care-A draft of the action plan,
the risk-disk and its manual, and a questionnaire were sent out to general practitioners and practice nurses for evaluation.
Results DUNDEE SCORE AND RANK
The box shows a formula for the multiple logistic
function with the modifications used for the Dundee
system. The effects of^ age, smoking, blood^ pressure,
and cholesterol concentration^ on^ coronary risk^ are^ all
highly significant, and there is^ a^ gradient in risk^ with
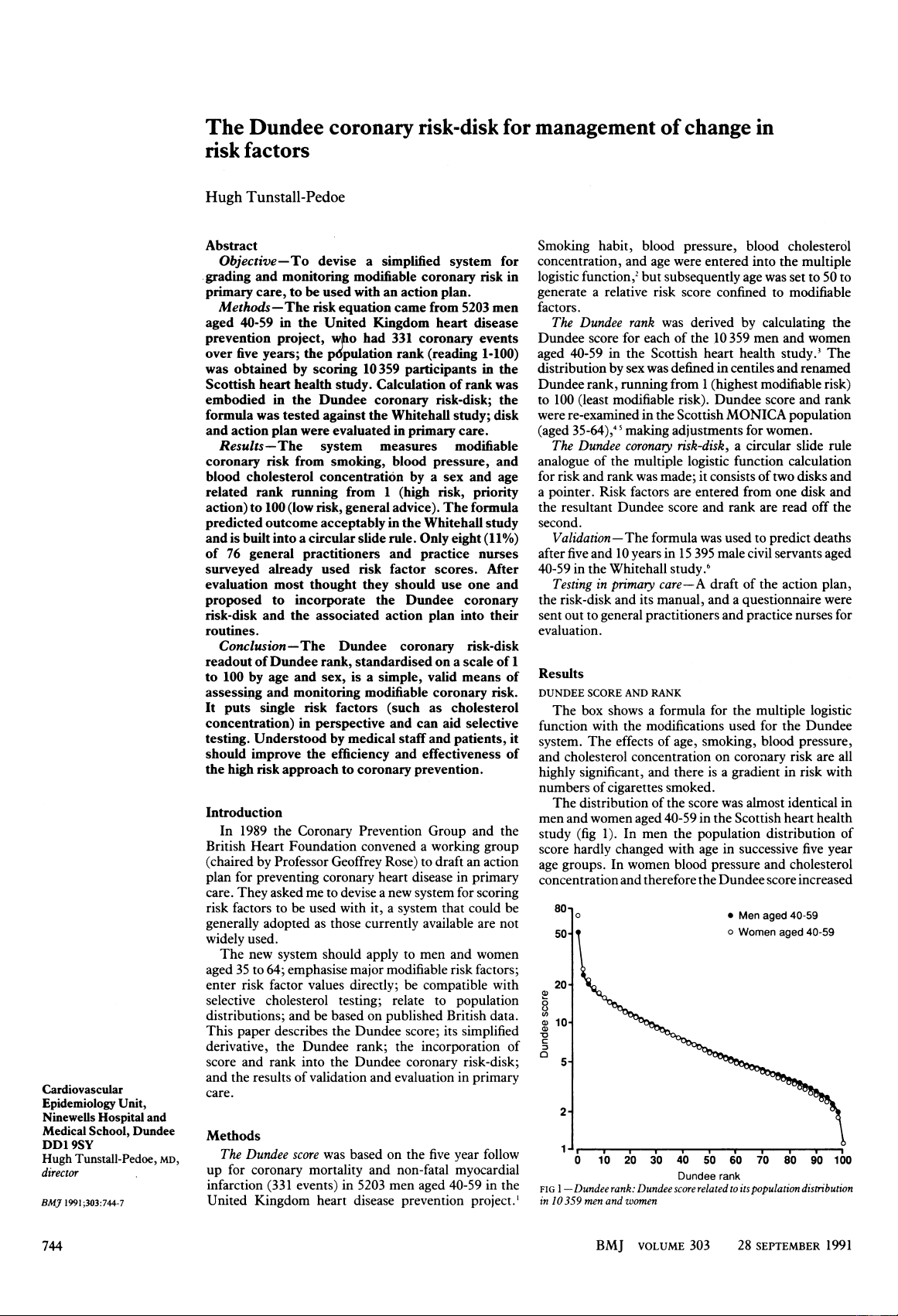
numbers of (^) cigarettes smoked. The distribution of the score was almost identical in men and women aged 40-59 in the Scottish heart health
study (fig 1). In men the population distribution of
score hardly changed with age in successive five year age groups. In women blood pressure and cholesterol concentration and therefore the Dundee score increased
80o0 *^ Men aged 40-
50- o^ Women^ aged 40-
20 0
a^ a10-
0 10 20 30 40 50 60 70 80 90 100 Dundee rank FIG 1-Dundee rank: Dundee score related to its population distribution in 10359 men and women
Multiple logistic function formula and modifications
Five (^) year risk (^) of coronary heart disease
l+e-(a + bix,^ + b2x2 + b3x3 + b4x4)
Coefficients (SEs) a = -10- (^117) (0-745) = constant*
b, =^ 0-06510^ (0-0114)^ xl^ =^ age^ in^ years*
b2 =^ 0-010543 (0^ 00270)^ x2^ =^ systolic^ blood^ pressure (mm Hg) b3 =^ 0-009378^ (0-00131)^ X3^ =^ cholesterol^ (mg/100 ml)** b4 =^1 00 X4= smoking^ code^ (see^ below)***
Smoking codes Never smoked =^ 0-0 (preset) Ex-smoker or pipe or cigar smoker =^ 0- 1453 (0-224) Cigarettes per day: 1-9 = 0-4483 (0-274) 20 10 = 0-9242 (0 283) 21- 11-19 = 1-019 (0 228) 330
Modificationsfor Dundee coronary risk-disk: *Constant "a" reset for fixed age 50: -10 117 + (50 x 0-0651) = -6-8624. This value is constant for men but is modified in women by age: 35 =^ +0-5719; 40 =^ +0 3875; 45 = +0- 1922; 50 =^ +0-0156; 55 =^ -0 1047; 60 =^ -0-2219; 65 =^ -^ 0-
**Cholesterol: b3= 0-3627; X3 =^ cholesterol (mmol/l)
***Cigarette dose-response rationalised to: 1-4/day = 0- 5-9/day =^ 0 406^ +^ (No of^ cigarettes -5)(0-08 13) 10-29/day = 0-8125 + (No of cigarettes - (^) 10) (0-0312) ¢30/day =^ 1-437.
= 1 263 (^) (0 303) = 1 431 (0 285)
rear notch is aligned with the front one, the zero point
for smoking habit. Risk factor values are entered in
turn by rotating both disks together through the
pointer by the appropriate amount, so that the rear
disk is rotated incrementally, from least risk towards
most risk, once for each risk factor. Blood pressure and
cholesterol concentration cannot be entered until they
have been zeroed on the pointer, which is done by
rotating the front disk alone through the pointer,
keeping the^ rear^ disk^ stationary. The sequence of
rotations is therefore line (^) up the disks, rotate both
disks together, move front disk only, rotate disks
together, move^ front disk only, rotate disks together,
read out from rear disk and pointer-potentially
confusing when^ first^ seen, but^ easily learnt and then
self evident.
with age. Before correction, the cut offpoint equivalent
to rank 15 would produce 15% of men in each five year age group 40-59, whereas in women it would produce 15% overall, but twice as many women aged 55-59 as
40-44. Score and rank are simpler if they have a
constant relation across age and sex groups. The
population data from the Scottish heart health study
and Scottish MONICA project were used to adjust the
scores for each age in women to give the best overall fit
to figure 1 for ranks 10, 15, 20, 25, and 50, the high risk
end of the distribution; this was achieved by adjusting
the multiple logistic function constant "a."
FIG 2-Front and rear views ofDundee coronary risk-disk
TABLE I-Deathsfrom coronary causes afterfive and l0years in 15 395 male civil servants aged 40-59 by decile ofDundee score
No (%) of deaths After 5 After 10 Decile of years years Dundeescore (n=195) (n=510)
1 8 (4) 18 (4) 2 10(5) 24 (5) 3 13 (7) 33 (6) 4 18 (9) 40 (8) 5 21 (11) 42 (8) (^6) 9(5) 37 (7) (^7 16) (8) 52 (10) (^8 21) (11) 56(11) (^9 29) (15) 84(16) (^10) 50(26) 124 (24)
DUNDEE CORONARY RISK-DISK
Initially the "Dundee coronary risk-disk" was
made and field tested as concentric card (^) disks. The
production version (fig 2) consists of two solid disks,
back to back, with coloured scales and a wrap around
pointer. The front disk is divided into segments for
smoking, blood pressure, and cholesterol scales. The
operator uses either the systolic or diastolic (phase V)
blood pressure. A supplementary cholesterol scale
shows mean British population levels by sex and age,'
so that a provisional Dundee rank can be assigned
while the operator considers whether cholesterol testing
is warranted. The rear disk contains concentric scales
for rank and score and the offsets by age for women.
The risk factor scales on the front are linear but the
score scale is almost logarithmic, reflecting multi-
plicative interaction of risk factors. Rank follows a
normal (^) or Gaussian distribution curve on the score
scale (fig 1), being crowded in the middle ranges and
spread out at^ the edges, where extreme scores are rare.
USE OF THE DISK
Except in^ women, for^ whom^ it^ is^ offset by age, the
VALIDATION Applied to the Whitehall study, the Dundee score produced the risk gradient shown in table I, placing in the top 20% of risk 41% of the 195 deaths from coronary heart disease after five years and 40% of the (^510) deaths after 10 years. The relative risk of those in the top versus bottom decile ofrisk was 6 3 in five years and 6 9 in 10 years.
TESTING IN PRIMARY CARE General (^) practitioners (and their (^) nurses) were recruited from a (^) cardiology course in Newcastle and (^) practice nurses (^) (and their (^) doctors) from (^) their conference in Perth. The (^) response from Newcastle produced 33 forms from (^) practitioners and 12 from nurses; that from Perth (^) produced 11 forms from doctors and 20 from nurses. After (^) inability to (^) partici- pate was corrected for the response rate (^) among Newcastle doctors was (^) 85%; the (^) response from Perth was less complete. Results were similar and were
combined in table II. Most respondents were carrying
out risk factor assessment or were about to do so, but
logistic function for systolic blood pressure. The project used diastolic phase IV readings, but phase V
readings should now be standard in Britain,'" so those
from the project have not been used. The diastolic equivalent for each systolic value is the reading that
occurred most commonly opposite it in the Scottish
heart health study.3 The risk-disk uses either systolic or phase V diastolic blood pressure.
CHOLESTEROL AND SELECTIVE TESTING
The argument for selective versus opportunistic
testing for cholesterol concentration is well known.'
The action plan lists unifactorial indications for
cholesterol testing.'3 In other cases a provisional
Dundee rank can be derived pending a decision on testing. The risk-disk can be used with any level of cholesterol testing. If a cholesterol result is available the Dundee rank places it in the context of overall modifiable risk. The contribution of cholesterol measurement to the Dundee rank was tested in the Scottish heart health study population by correlating the provisional Dundee rank with^ the final one. Seventy per cent of subjects remained (^) within the same risk decile or the one
adjoining it.
WOMEN The use of a relative risk score, (^) together with the observation that risk factor distributions in men and
women aged 40-59 are similar, means that the Dundee
score and rank can be used for women as well as men.
The weightings given to the three factors are derived
from men. Absolute risk in women is lower, but
despite' the anomalous results on smoking from
Framingham,2 the major risk factors seem to operate,
and may be weighted similarly, in both sexes (un-
published data). Using the Dundee system for women
is reasonable provided that users remember that score and rank are relative to that age and sex-a Dundee rank of 5 is far more threatening over five years to a man of 60 than to a woman of 40. The offset by age in
women is to ensure that equal proportions exceed
preset cut off points. Altering the offset does not affect relative risk relations within an age group because the
score is^ logarithmic.
POTENTIAL FOR THE DUNDEE (^) CORONARY RISK-DISK AND DUNDEE RANK Measurement ofrisk is not an end in (^) itself but (^) should
be undertaken to improve patient management, to find
those who stand to benefit most, and to motivate staff
and patients. Otherwise the workload in risk factor
counselling could be overwhelming.'
Current commercial interest in coronary risk is
centred largely on lipids. There is a popular impression
that cholesterol is all important and that coronary
risk can be (^) expressed in cholesterol units. The
Dundee coronary risk-disk, through risk rank, has an
educational role in putting cholesterol in perspective
and emphasising interaction: cholesterol is not the only
risk factor, and the risk attributable to a high reading
depends on the levels of other factors. 16
It may be ambitious to expect that the risk-disk will
be adopted in most or even a substantial minority of
practices assessing coronary risk factors. The adoption ofa single standard would, however, have considerable advantages. Coronary risk could be discussed, measured, and tracked independently of any single risk factor. The Dundee rank has that potential: in classifying patients on a scale of 1 to 100 in terms of modifiable risk and, in lay terms, telling patients how far (^) they are from the (^) front of the coronary queue.
In addition to the members of the working (^) group respons- ible for the action plan, I thank for help, ideas, and criticisms the doctors and nurses involved in formal and informal evaluations; Dr Simon Thompson and Mr Martin (^) Shipley (London); Professor Gino Farchi and Dr Susanna Conti (Rome); the staff of Gerrard and Medd, designers (Edinburgh); the Coronary Prevention Group (London); and the cardiovascular epidemiology unit (Dundee). The Dundee unit is funded by the Scottish Home and Health Department; views expressed in this paper are my own. Financial help is acknowledged from a Toshiba Year of Invention award, the British Heart lioundation, the Health Education Board for Scotland, and Dundee University. The Dundee coronary risk-disk (UK registered design No 2 011 353) is supplied with an illustrated manual at a unit price ofF 15 (including VAT) plus £3 handling charge for each order (1-49 disks). An educational videocassette, software program, full price list, and further information are also available from: Risk-Disk, CVEU, Ninewells Hospital, Dundee DD1 9SY. Potential users must be prepared to spend the time necessary for familiarisation and simple testing to prevent error; the^ suppliers disclaim responsibility for misuse in practice.
1 Rose G, Tunstall-Pedeo H, Heller RF. UK heart disease prevention project: incidence and mortality results. Lancet 1983;i: 1062-5. 2 Chambless LE, Dobson A, Patterson CC, Raines B. On the use ofa logistic risk score in predicting risk of coronary heart disease. Statistics in Medicine 1990;9:385-96. 3 Smith WCS, Tunstall-Pedoe H, Crombie IK, Tavendale R. Concomitants of excess coronary deaths-major risk factor and lifestyle findings from 10 359 men and women in the Scottish heart health study. Scot Med J 1989;34: 550-5. 4 World Health Organisation MONICA Project Principal Investigators (Pre- pared by Tunstall-Pedoe H). The World Health Organization Monica Project (Monitoring trends and determinants in cardiovascular disease): a major international collaboration. J^ Clin Epidemiol 1988;41:105-14. 5 Smith WCS, Shewry MC, Tunstall-Pedoe H, Crombie IK, Tavendale R. Cardiovascular disease in Edinburgh and north Glasgow-a tale of two cities. J Clin Epidemiol 1990;43:637-43. 6 Jarrett RJ, Shipley MJ, Rose G. Weight and mortality in the Whitehall study. BMJ7 1982;285:535-7. 7 Tunstall-Pedoe H, Smith WCS, Tavendale R. How-often-that-high graphs of serum cholesterol. Findings from the Scottish heart health and Scottish MONICA studies. Lancet 1989;i:540-2. 8 British Hypertension Society Working Party. Treating mild hypertension. BMJ (^) 1989;298:694-9. (^9) European Atherosclerosis (^) Society Study Group. Strategies for the prevention of coronary heart disease: a (^) policy statement of the (^) European Atherosclerosis Society. EurHeartJ^ 1987;8:77-88. 10 Thorsen RD, Jacobs (^) DR, Grimm RH. Preventive (^) cardiology in (^) practice: a device for risk estimation and (^) counselling in (^) coronary disease. (^) Prev Med 1979;8:548-56. 11 Shaper AG, Pocock (^) SJ, Phillips AN, Walker M. A (^) scoring system to (^) identify men at high risk of a heart attack. Health Trends 1987;19:37-9. 12 Heller RF, Chinn S, Tunstall-Pedoe (^) HD, Rose G. How well can we (^) predict the development of coronary heart disease? Findings in the UK heart disease prevention project. BMJ 1984;288:1409-11. 13 Coronary Prevention Group and British Heart Foundation. Action (^) plan for preventing coronary heart disease in primary care. BMJ 1991;303:748-50. 14 Lee AJ, Smith WCS, Lowe GDO, Tunstall-Pedoe H. Plasma fibrinogen and coronary risk factors: the Scottish heart health study. 7 Clin Epidemiwl 1990;43:913-9. 15 Petrie JG, O'Brien ET, Littler WA, de Swiet M. Recommendations on blood pressure measurement. BMJ 1986;293:611-5. 16 Tunstall-Pedoe H. Who is for cholesterol testing? BMJ 1989;298:1593-4. 17 Imperial Cancer Research Fund OXCHECK Study Group. Prevalence of risk factors for heart disease in OXCHECK trial: implications for screening in primary care. BMJ 1991;302:1057-60. (Accepted 20 August (^) 1991)