

NURSING EDUCATION AND
THE PATH TO POPULATION
HEALTH IMPROVEMENT
MARCH 2019






































Study with the several resources on Docsity

Earn points by helping other students or get them with a premium plan

Prepare for your exams
Study with the several resources on Docsity
Earn points to download
Earn points by helping other students or get them with a premium plan
Community
Ask the community for help and clear up your study doubts
Discover the best universities in your country according to Docsity users
Free resources
Download our free guides on studying techniques, anxiety management strategies, and thesis advice from Docsity tutors
Nurses are in schools, workplaces, homes, prisons, hospitals, assisted living facilities, and other community spaces. They practice where people live, work, and ...
Typology: Lecture notes
1 / 48

This page cannot be seen from the preview
Don't miss anything!
he United States outspends every country on health care, yet its residents have shorter lives and poorer health (IOM, 2013; Sawyer and Gonzalez, 2017; Commonwealth Fund, 2015). Further investigation of this phenomenon demonstrates that it is related, in large part, to a lack of universal access to care and a lack of attention to the social determinants of health— those conditions affecting health where people live, learn, work, and play (WHO, 2008). The Robert Wood Johnson Foundation (RWJF) recognized this and began to address it with its Culture of Health Action Framework, to move the nation toward health, equity, and well-being (RWJF, n.d.). The framework calls for making health a shared value, fostering cross-sector collaborations, creating healthier, more equitable communities, and strengthening integration of health services and systems, all leading to improved population health outcomes. The nation’s nurses are key players in moving the nation to a Culture of Health_._ Nursing is the largest and most trusted health profession, one that is historically embedded in every part of the health care system and community. Nurses are in schools, workplaces, homes, prisons, hospitals, assisted living facilities, and other community spaces. They practice where people live, work, and learn and where people attain, regain, and maintain their health. They are poised to lead efforts to improve the health and well-being of individuals, families, communities, and the population now and in the 21st century. In 2017, RWJF brought together a group of thought leaders to explore the key roles that nurses play in improving the health of the U.S. population. These explorations resulted in the report Catalysts for Change: Harnessing the Power of Nurses to Build Population Health in the 21st Century (Storfjell et al., 2017). The Catalysts report recommended that nursing and health care move beyond the individualistic, downstream focus of traditional medical care, and rather view individuals and families in the context of their environment to assess “how their community affects them.” Using the report as a springboard, RWJF commissioned a two-phase project, Population Health in Nursing, or PHIN, to explore promising models of nursing education and practice related to improving population health. The goal of the first phase, PHIN 1, was to describe promising educational models to prepare nurses, across all levels of professional practice, for population health practice and leadership. The second phase, PHIN 2, will describe current and emerging nursing roles in population health practice and how nurses should be prepared for these roles. PHIN 1 has been completed. A brief synthesis of the methods, findings and implications follow. Detailed information on PHIN 1 methods, findings and implications are included in the full report. PHIN 2, describing current and emerging nursing roles in population health practice and how nurses should be prepared for these roles, will begin in February 2019.
nursing education curricula, there are also significant challenges. Faculty practice and student clinical models that are embedded in the community have the potential to benefit both students and the population. However, there is little experience in measuring student learning outcomes. In addition, little work has been done measuring the impact of student and faculty efforts on population health outcomes. Also, many faculty members are not prepared in population health (practice and/or education), so they are not able to conceptualize population health and then integrate it into curricula.
Respondents to the survey and interviews with leadership and faculty at the site visits all recommended that population health be threaded through all levels of nursing education. While several schools are using creative teaching methods, integration of population health into nursing curricula cannot be accomplished without intentional, structured, mutually beneficial academic-practice partnerships; significant faculty development in population health practice and education; and the development of metrics to assess student competence in population health and their impact on population health outcomes. Enhancing students’ competence in population health is an important first step in strengthening the capacity of the nursing workforce to build a Culture of Health.
To build on PHIN 1 findings, next steps include ■ (^) Discussing with professional nursing education organizations ways to encourage curricular change. ■ (^) Exploring measures of population health competency that can be used across all nursing programs, based on level of nursing education. ■ (^) Continuing to explore successful IPE models as they relate to population health competencies. ■ (^) Identifying PHIN 1 lessons learned to inform PHIN 2 goals and methods. ■ (^) Bringing together thought leaders in nursing and health professional practice and education to 1) reflect on PHIN 1 findings and implications for nursing education; 2) advise on goals, methods, and key informants for PHIN 2 focus on nursing practice in population health; and 3) discuss strategies for preparing all health professionals to improve population health and thus build a vibrant Culture of Health in America.
Commonwealth Fund. (2015). The Affordable Care Act’s Payment and Delivery System Reforms: A Progress Report at Five Years. Retrieved from ( https://www.commonwealthfund.org/publications/ issue-briefs/2015/may/affordable-care-acts-payment- and-delivery-system-reforms ). Institute of Medicine (IOM). (2013). Shorter lives, poorer health: US health in international perspective. Washington, DC: National Academies Press. Robert Wood Johnson Foundation (n.d.) Culture of Health. Retrieved from https://www.rwjf.org/en/ how-we-work/building-a-culture-of-health.html World Health Organization (WHO), Commission on Social Determinants of Health, 2005-2008. Retrieved January 2018 from https://www.who.int/ social_determinants/thecommission/en/ Sawyer, B. and Gonzalez, S. (2017, May 2017). How does the quality of the US health care system compare to other countries? Retrieved from Kaiser Family Foundation https://www. healthsystemtracker.org/chart-collection/quality-u-s- healthcare-system-compare-countries/#item-mortality- rate-cancers-falling-u-s-across-comparable-countries. Storfjell, J., Winslow, E. and Saunders, J. (2017). Catalysts for Change: Harnessing the Power of Nurses to Build Population Health in the 21st Century. Robert Wood Johnson Foundation. Retrieved from https://www.rwjf.org/content/dam/ farm/reports/reports/2017/rwjf
he United States outspends every country on health care, yet its residents have shorter lives and poorer health (IOM, 2013; Sawyer and Gonzalez, 2017; Commonwealth Fund, 2015). Further investigation of this phenomenon demonstrates that it is related, in large part, to a lack of universal access to care and a lack of attention to the social determinants of health—those conditions that have an impact on people’s health where they live, work, and play (WHO, 2008). The Robert Wood Johnson Foundation (RWJF) recognized this and began to address it with its Culture of Health Action Framework, to move the nation toward health equity and well-being (RWJF, n.d.). This framework calls for making health a shared value; fostering cross-sector collaboration; creating healthier, more equitable communities; and strengthening integration of health services and systems, all leading to improved population health, well-being, and equity. Key players in moving America to a Culture of Health will be the nation’s nurses_._ Nursing is the largest and most trusted health profession, one that is historically embedded in every part of the health care system and community. Nurses are in schools, workplaces, homes, prisons, hospitals, assisted living facilities, and other community spaces. They practice where people live, work, and play; where people attain, regain, and maintain their health. They are where the needs are greatest for a population-focused system of health and wellness. In response to the need to improve the health of our nation by creating a Culture of Health, and reflecting the importance of nursing in the health care system and in community health, the Robert Wood Johnson Foundation produced the paper Catalysts for Change: Harnessing the Power of Nurses to Build Population Health in the 21st Century. That 2017 report (Storfjell et al., 2017) asked: How can nurses best help our nation reverse course on the declining health of its residents and promote the health of the U.S. population in the 21st century? The Catalysts paper contended that nursing must move beyond the individualistic, downstream approach of traditional medical care, to rather view individuals and families in the context of their environment and assess “how their community affects them.” Using the Catalysts report as a springboard, RWJF commissioned a study to identify best practices in educating nurses in basic population health knowledge and skills across levels of professional practice, to prepare them to be key players in creating a Culture of Health. The study is called Population Health in Nursing (PHIN).
The first phase of the PHIN study, PHIN 1, was conducted using the following methods. The first method was a survey of a convenience sample of practice leaders and faculty in nursing, public health, and social work. The second method included in-depth interviews with 26 nursing and public health leaders recommended in the survey results. The third method consisted of site visits to
incentive for their participation. Interviews were conducted between May 17 and June 1, 2018. Afterward, Alan Newman Research provided transcripts, a summary, and an analysis to the PHIN study team. The interviews were tailored to solicit perspectives of educators and health care leaders on what nurses needed to know in population health and how it could best be taught. The interviews addressed the following content areas: ■ (^) Level(s) of students to include in an ideal program (associate degree—ADN; baccalaureate degree—BSN; master’s degree—MSN; clinical doctorate in nursing practice—DNP; advanced public health nursing—APHN; advanced practice registered nurse—APRN). ■ (^) Intended goals or outcomes of population health education. ■ (^) Benefits of population health education, i.e., ways in which it would contribute to improved health outcomes, as well as benefits to nursing students and to the school. ■ (^) Key content and areas of focus, specific subject matter, skills, and core courses to include. ■ (^) Teaching methods, clinical experiences and learning activities, interactions with other health professionals, and other health professions students that should be included. ■ (^) Faculty qualifications for teaching population health. ■ (^) Evaluation methods to assess nursing students’ knowledge and skills in population health. ■ (^) Educators’ satisfaction with their current population health program/content. ■ (^) Challenges and barriers to offering a population health program. ■ (^) Suggestions to enhance effectiveness in teaching population health to nursing students. ■ (^) Real-world strategies that are effective in applying population health concepts.
The PHIN study team selected six programs that had been identified by the nursing and population health leaders via the survey or in-depth interviews as exemplar nursing education programs in population health. The team then scheduled one- and-a-half-day site visits with each program to collect additional data on curricular initiatives, practice experiences, administrative support for the educational initiatives, as well as student perspectives on the curricula. (See Appendix C for a typical site visit schedule.) Each school was contacted with a request to participate in a site visit, and visits were scheduled between July and October
The findings from each phase in the study are presented below. Similar questions and topic areas were explored during all three phases of the study. The study was designed to increase—with each method of data collection—the depth and complexity of the responses. The findings are divided into the following organizing themes: 1) Key content including core concepts and skills for population health; 2) teaching methods; 3) benefits and challenges to incorporating population health in nursing curricula; and 4) identification and measurement of
The 66 respondents provided a broad overview of current key concepts and practices in public and population health. For non-nurse respondents, the survey questions did not include details about the degrees earned and the level of nursing education. Rather, those outside the profession were asked to identify the importance of core content in population health for a generalist professional nurse (BSN). AARP Research conducted data analysis and results were shared with the PHIN study team.
44% nursing or public health educator 24% nurse practitioners 32% other (e.g., general educator, public health professional, medical professional)
0 5 10 15 20 25 30 schools of nursing higher education/ university government/ nonprofit organizations PERCENTAGE
0 10 20 30 40 50 60 70 80 PERCENTAGE10+ years in current position 20+ years in workforce
0 20 40 60 80 100 nurses non-nurses PERCENTAGE
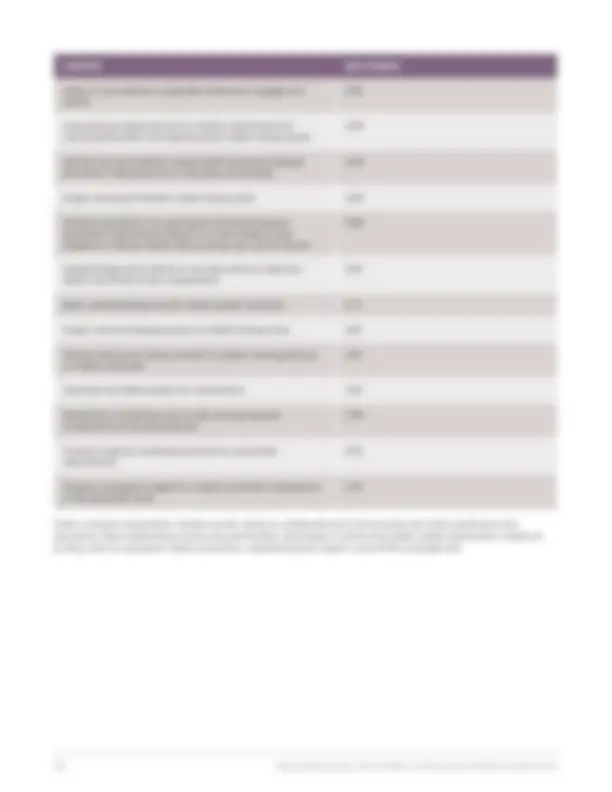
CONTENT ADN BSN MSN DNP/APRN DNP/APHN Develop population-focused health promotion/ disease prevention interventions based on current evidence and targeted to relevant health literacy levels and cultural factors 1.76 2.44 2.81 2.81 3. Basic understanding of public health system functions 2.36 2.79 2.86 2.93 3. Describe cost effectiveness for interventions 1.67 2.16 2.76 2.90 3. Conduct capacity-building assistance for population interventions 1.16 1.74 2.45 2.60 3. Understand the impact of health policy on nursing practice and health outcomes 2.08 2.67 2.91 2.95 3. Identify avenues for policy activism to impact nursing practice or health outcomes 1.79 2.42 2.81 2.91 3. Develop a program budget for a health promotion intervention at the population level 1.11 1.81 2.56 2.63 3. Other concepts respondents named include: demonstrate public health nursing competence in practice; Identify gaps in evidence for successful programs; Institute of Medicine occupational and environmental health competencies for nursing; networking/social skills; partner with communities/populations to improve health; see themselves as leaders in population health; understand precepts of building a Culture of Health; understand the impact of health system financing; utilize community-based participatory methods for assessment, implementation, and evaluation Table 2 presents survey findings from the perspective of non-nurses on the importance of specific content topics for nursing education. Non- nurse respondents were asked their views on population health knowledge and skills of most importance for nursing practice at the level of the generalist professional nurse (BSN). TABLE 2: IMPORTANCE OF SPECIFIC CONTENT IN NURSING CURRICULUM AT BSN LEVEL: NON-NURSE RESPONDENTS (1–3: LOW TO HIGH IMPORTANCE) CONTENT NON-NURSES Refer/intervene to address social determinants of health (SDOH) with significant health impacts for individuals and families
Understand the impact of health policy on nursing practice and health outcomes
Ability to use evidence supported methods to engage with communities/populations
Assess individuals/families for SDOH 2.
CONTENT NON-NURSES Ability to use evidence-supported methods to engage with clients
Use evidence-based practice to modify interventions for individuals/families to be appropriate to health literacy levels
Identify and use evidence-based health promotion/disease prevention interventions for individuals and families
Assess individuals’/families’ health literacy level 2. Develop population-focused health promotion/disease prevention interventions based on current evidence and targeted to relevant health literacy levels and cultural factors
Epidemiology basics (ability to use basic terms to describe health and illness across a population)
Basic understanding of public health system functions 2. Assess communities/population for health literacy level 2. Identify avenues for policy activism to impact nursing practice or health outcomes
Describe cost effectiveness for interventions 2. Biostatistics (understand use of rates and appropriate comparisons across populations)
Conduct capacity-building assistance for population interventions
Develop a program budget for a health promotion intervention at the population level
Other concepts respondents named include: ability to collaborate and communicate with other professions and disciplines; lead collaborative community partnerships; participate in community health needs assessments; impact of primary care on population health outcomes; understand public health nurse (PHN) competencies
BENEFIT PERCENTAGE OF RESPONDENTS Student interest 29.7 percent Accreditation requirements 18.8 percent Licensure expectations 10.9 percent Other concepts respondents named include: develop change agents, empower nurses to improve communities, create a Culture of Health; help focus efforts on health rather than illness care; improve patient/population health outcomes; answer need to address health disparities and SDOH; once students understand population health concepts and skills, they apply this lens to the care they provide wherever they work, to the benefit of patients; promote impact of primary intervention on health care outcomes; relevant to quality of care; stay ahead of the changes in health care Table 5 documents respondents’ perspectives on the top challenges to teaching nursing students about population health. The top challenge identified by 65.6 percent of respondents was faculty expertise. Respondents also named as challenges the availability of appropriate clinical experiences (50 percent) and support of current faculty (42.2 percent). Additional challenges that individual respondents identified were lack of resources; lack of clear outcomes; burdensome institutional standards; and lack of National Council Licensure Examination-RN (NCLEX) content. TABLE 5: THREE TOP CHALLENGES TO EDUCATION IN POPULATION HEALTH CHALLENGES PERCENTAGE OF RESPONDENTS Faculty expertise 65.6 percent Availability of appropriate clinical experiences 50 percent Faculty support 42.2 percent Licensure expectations 29.7 percent Lack of time 25 percent Student interest 17.2 percent Relevant job opportunities 12.5 percent Accreditation requirements 10.9 percent There are no challenges 3.1 percent Other concepts respondents named include: available resources; lack of clear outcomes; curriculum is already too “stuffed”; faculty experience; increased need for institutional requirements beyond the standard fingerprints, immunizations, etc., for students; lack of accreditation requirements; lack of support for and interest in population health across the curriculum (not seen as important); NCLEX; nursing culture (in practice and in academic settings) values acute care and specialization over public health; prioritizing medical model over health for all; APRNs with limited vision; social and cultural divisions between nurse students and relevant communities
Respondents were asked to identify ways to measure nursing student competency/knowledge in population health, on a scale of 1 to 5. The results are outlined in Table 6. Note: For this, the lower the number, the higher the importance of the measure (1 is “very important”). The most important measure of student competency was “valid and reliable end-of-program population health competency assessment.” Case studies with multiple choice or essay responses; course grades in relevant courses; and clinical preceptor evaluation of student performance were identified as slightly less important. Skills checklist was identified as the least important measure. TABLE 6: IMPORTANCE OF SUGGESTED MEASURES OF NURSING COMPETENCY IN POPULATION HEALTH (1–5: HIGH-TO-LOW IMPORTANCE) SUGGESTED MEASURES IMPORTANCE Valid and reliable end of program population health competency assessment
Valid and reliable population health case studies— multiple choice or essay responses
Course grades in relevant courses (e.g., epidemiology, biostatistics, public health nursing, health policy, etc.)
Clinical preceptor evaluation of student performance 2. NCLEX completion 3. Role playing with observational assessment 3. Employer assessment 3. Skills checklist 3. Other concepts respondents named include: faculty evaluation of population health clinical projects; if hospitals and health systems integrated SDOH screening and intervention by nursing, nursing colleges/schools would teach those concepts; population health included in NCLEX; portfolio of community and population change projects 2: IN-DEPTH INTERVIEWS The in-depth interviews focused on gaining more information on the same topics included in the survey from respondents with more knowledge in population health. The findings from these interviews are provided using the same four organizing themes described in the survey findings above. Respondent Characteristics Interviewees included 15 leaders (six nursing, four public health, two population health, one medicine, and two public health nursing) and 11 nurse educators. They represented a variety of organizations— including national nursing associations and councils; large health care systems; the Centers for
According to participants, there are a number of potential challenges related to offering a population health nursing program. In general, perceived challenges related to an overall lack of awareness, understanding, and prioritization of population health in general—as well as to the logistics of offering a population health program. Specifically, participants mentioned: ■ (^) Difficulty changing the status quo as it relates to teaching nursing (i.e., the focus on acute setting and individual patient care). ■ (^) Competing priorities and lack of awareness, understanding, and prioritization of population health content by administrators, faculty, and students. ■ (^) Lack of qualified faculty to teach population health and requirement that nursing faculty be nurses themselves. ■ (^) Difficulty finding appropriate sites for clinical placements and restrictive related rules and licensing requirements. ■ (^) Already crowded nursing curricula. ■ (^) Lack of/limited inclusion of population health content on the NCLEX (which contributes to de-prioritization). ■ (^) Logistical challenges related to interprofessional education. Participants offered a number of suggestions to overcome these challenges and enhance effectiveness in teaching population health to nursing students: ■ (^) Provide professional development to existing faculty—webinars, expert presentations, roundtable discussions. ■ (^) Develop resources, materials, and a toolkit to help educators develop or expand their population health curriculum—include suggested curriculum and core content; ways to embed content in existing courses; specific assignments; examples of clinical sites; best practices and advice. ■ (^) Offer online forums, bulletin boards, or other convenient means to interact with nurse faculty or administrators teaching population health across the country. ■ (^) Broaden the definition of approved sites for clinical rotations and what counts as clinical hours. ■ (^) Add or expand population health-related questions on the NCLEX. ■ (^) Provide population health-related professional development opportunities and additional schooling to licensed, practicing nurses. ■ (^) Ensure nurses at all levels, including ADN, are exposed to population health content. ■ (^) Begin teaching population health concepts early in the nursing curriculum, addressing basic population health concepts and skills. ■ (^) Expand opportunities for experiential learning and interprofessional education and interaction. ■ (^) Develop communications initiatives regarding the importance and relevance of population health, targeted to faculty and administrators of nursing schools, students, and employers. ■ (^) Create expanded national awareness of the key role of nurses (not just physicians) in population health. ■ (^) Offer grants, monetary incentives, or start-up money to nursing schools that offer a graduate program in population health. ■ (^) Provide grants to students studying population health to help offset tuition costs. Leaders identified some real-world strategies that are effective in the application of population health concepts. ■ (^) Technology-related strategies include use of electronic health records in various ways to identify populations and communicate with them; text reminders to patients; wearable health monitors; telehealth; e-visits with physicians and pharmacists; and geomapping and use of other data sets. ■ (^) Participants currently work in partnership with a variety of community organizations to address a number of issues. Examples include public health departments; local government; business organizations; nonprofits; citizen coalitions; law enforcement; churches; and insurers.
■ (^) Community resources that are utilized include websites and searchable databases to find community partners and resources for patients as well as grant money for interventions and studies.
Nursing knowledge in population health is evaluated in a number of ways, depending on the course objectives and level of students. Measurement of student outcomes and competencies was identified as a particularly challenging task. Regardless of the specific method used, students’ ability to understand and apply the concepts must be assessed. 3: SITE VISITS A data summary table for all site visits categorized by the organizing themes is provided below (Tables 7–10). In addition, a brief summary of the most notable findings from each site visit is included.
Based on the responses from the surveys and in- depth interviews, six nursing educational programs were selected for site visits, to provide the opportunity to look at teaching content and methods currently being implemented, discuss challenges and lessons learned, and see how students respond to curricula in population health. Schools selected included: ■ (^) Oregon Health & Science University ■ (^) Rush University ■ (^) Rutgers University ■ (^) Thomas Jefferson University ■ (^) University of North Carolina ■ (^) University of Washington
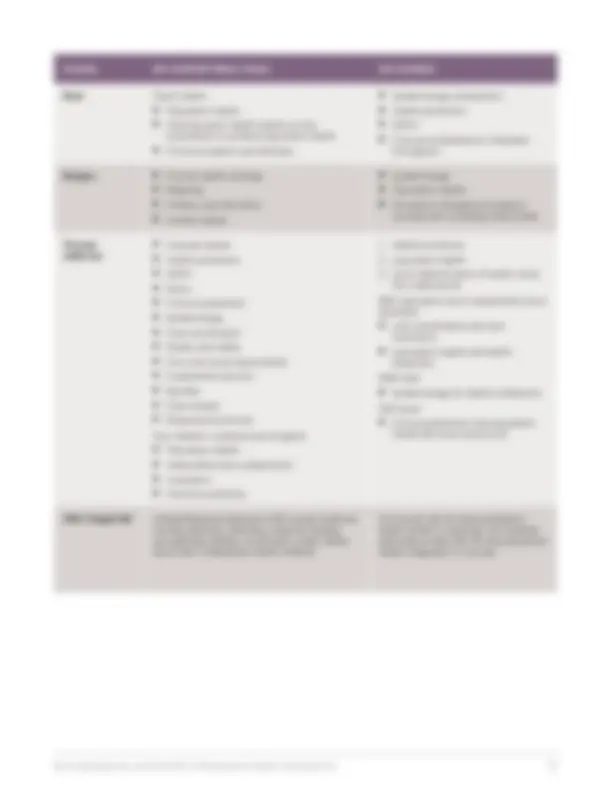
The key content and courses, including core concepts and skills for population health identified in the site visits are outlined in Table 7 below. The findings at the site visits reinforced the importance of the content areas of epidemiology, population health, and SDOH and illustrated different strategies for incorporating this content. TABLE 7: KEY CONTENT AREAS/COURSES AT SITE VISIT PROGRAMS SCHOOL KEY CONTENT AREAS, TOOLS KEY COURSES Oregon Health & Science University ■ (^) Population health ■ (^) SDOH ■ (^) Epidemiology ■ (^) Mentorship ■ (^) Resource management ■ (^) Quality improvement ■ (^) One of 10 competencies Population health is threaded throughout as one of the key competencies in the entire curriculum.