Arrhythmias and Cardiac Emergencies
Sandra Goldsworthy, David Waters
CHAPTER ELEVEN
}
LEARNING OUTCOMES
After completing this chapter you will be able to:
• Systematically interpret sinus, atrial, junctional, ventricular and
heart block rhythms.
• Describe nursing implications and treatment for sinus, atrial,
junctional, ventricular and heart block rhythms.
• Describe priority treatment for key cardiac emergencies such
as cardiac arrest.
• Test your knowledge with practice questions and a case study
at the conclusion of the chapter.
INTRODUCTION
Arrhythmia interpretation and care of patients experiencing acute
cardiac events is a foundational competency required of registered
nurses working in critical care. The aim of this chapter is to provide
a resource for critical care nurses internationally that will assist
with recognition of key characteristics of sinus, atrial, junctional,
ventricular arrhythmias and atrio-ventricular (AV) blocks. In addition,
evidence-based care will be discussed in relation to symptomatic
arrhythmias and cardiac emergencies such as myocardial infarction
and cardiac arrest.
The chapter will conclude with practice questions and a case
study. Helpful websites and further resources will also be provided.
The intention of the chapter is to provide an overview of the key
components of basic arrhythmias and a summary of treatment. The
chapter is designed to accommodate learners that have a good
understanding of cardiac anatomy and physiology in addition to an
introductory level of understanding of cardiac arrhythmias.
Arrhythmia interpretation: where to start
The first part of accurately interpreting arrhythmias is to use a
systematic approach (see Table 1). However, before you begin to
analyze the rhythm strip, ALWAYS check the patient first and ensure
they are stable.
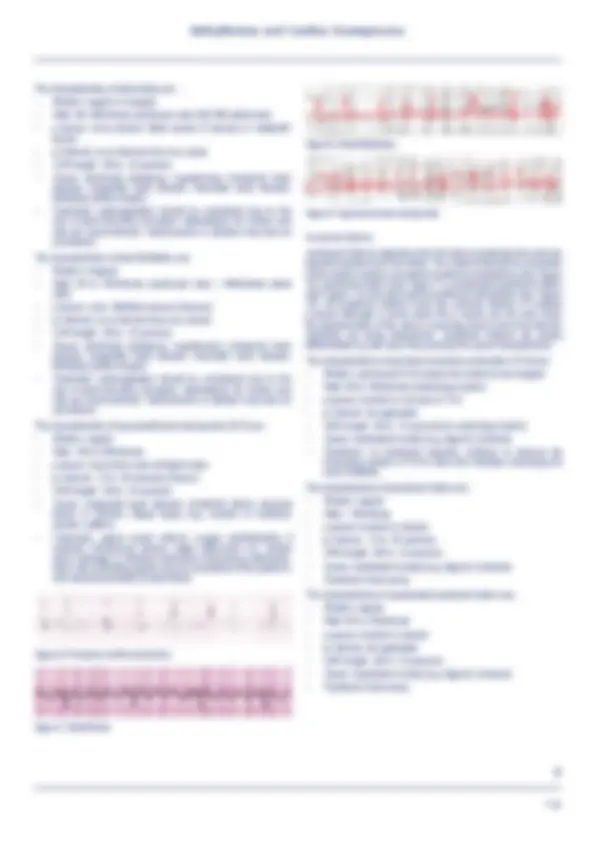
Normal sinus rhythm
In order to analyze cardiac rhythms, it is essential to have an
understanding of the ‘benchmark’ rhythm or hemodynamically
perfect rhythm; which is referred to as normal sinus rhythm (see
Figure 1) and sometimes abbreviated to NSR.
Figure 1. Normal sinus rhythm
In order to be considered normal sinus rhythm, the rhythm must have
the following characteristics:
Steps Explanation
1. Regularity Assess whether the rhythm is
regular or irregular
2. Rate Calculate ventricular and atrial rate
3. Assess p waves Are the p waves: rounded,
symmetrical, one for every QRS,
all look the same?
4. Calculate pr interval Normal =.12 to .20 seconds
5. Calculate QRS interval Normal = .06 to .10 seconds
6. Assess ST segment The ST segment should be on the
baseline or ‘isoelectric’ line. If it
is elevated or depressed it could
mean cardiac injury or ischemia
and requires urgent further
assessment.
In addition, the physician should
be notified immediately since
this could indicate that the
patient could be experiencing a
myocardial infarction.
7. Interpret the arrhythmia Name the arrhythmia based on the
characteristics above (i.e. atrial
fibrillation)
8. Nursing intervention/
treatment required
Determine what intervention is
required.
Is the patient stable or unstable?
Should the physician be notified?
Table 1. Systematic approach to arrhythmia interpretation
• Rhythm: regular
• Rate: 60 to 100/minute
• p waves: present, upright, symmetrical, one before every QRS
• pr interval: .12 to .20 seconds
• QRS length: .06 to .10 seconds
If the rhythm has all of the above characteristics but the ST segment
is elevated, it would be referred to as sinus rhythm with an elevated
ST segment versus ‘normal’ sinus rhythm.
Sinus rhythms
In the next section, arrhythmias originating in the sino-atrial (SA)node
will be explored. The characteristics, causes, nursing implications
and treatment required for sinus bradycardia, sinus tachycardia,
sinus arrhythmia and wandering atrial pacemaker will be presented.
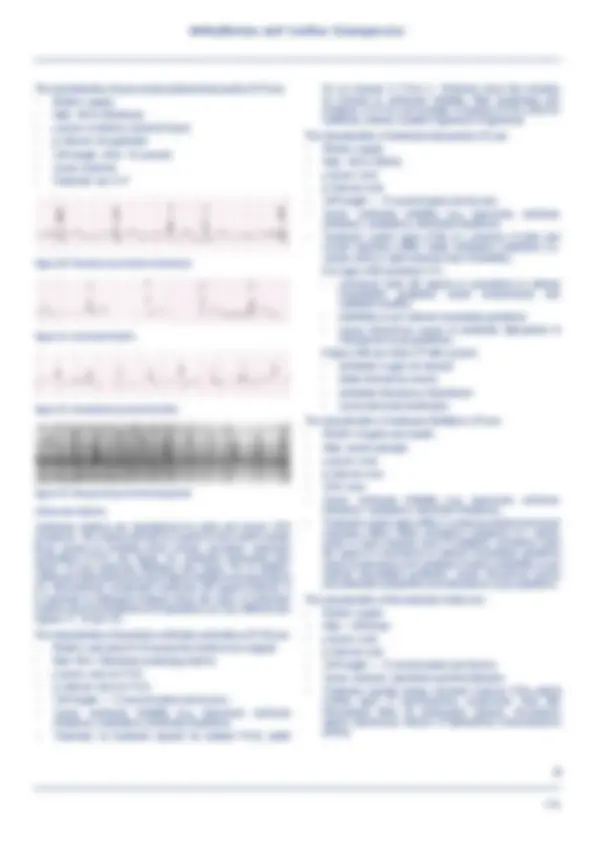
Slow rhythms: sinus bradycardia
A patient is considered to be bradycardic when their heart rate drops
below 60 beats per minute. Generally, a person often becomes
symptomatic when their heart rate drops below 50 beats/minute,
(see Figure 2) however slower heart rates can be observed in fit
and athletic individuals, who will often remain asymptomatic. As a
113